
In parts one and two of our series on breastfeeding problems, our midwife Katrin Ritter explained what makes a good start to breastfeeding and how correct latching on works. But what happens if you still can’t cope or you have one or two other problems? In hospitals there are often trained breastfeeding counsellors (IBCLC) who have thorough training and can help you. Otherwise, of course, a midwife with breastfeeding experience, or breastfeeding support networks can always help. Here are some of the most common reasons for early weaning.
What can have a negative effect on breastfeeding:
- Oxytocin administration during birth as a medicine: this can disrupt the maternal oxytocin system, but also have an influence on the baby’s reflexes and immune system.
- Painkillers (opioids) and anaesthesia for the mother.
- A surgical delivery, by caesarean section. Possible consequences: You need rest and limited movement for recovery and tend to lie on your back at first, so your hormone balance is affected.
- Artificial teats, nipples and soothers. If possible, avoid them completely for the first 4 to 6 weeks to prevent feeding confusion.

Is it normal to have pain when breastfeeding?
Some women stop breastfeeding because they feel pain. But is that actually normal? And how much do we have to put up with? In the first few days, you will have pain while breastfeeding. This can last for a few days and is intensified by the fact that oxytocin, which promotes labour, is released during breastfeeding. In addition, the nipples may be sensitive and slightly sore at most during the first two to three days. In the first one to three weeks, there may be pain at the beginning of the breastfeeding session for 20 to 30 seconds until the milk-supply reflex sets in. This is a pulling sensation in the nipples and breasts and is considered normal. After that, the pain should stop.
However, there are some reasons why breastfeeding may cause you persistent pain or otherwise not work properly. In these cases, it is important to talk to your midwife or breastfeeding consultant.
The most common breastfeeding problems in early labour
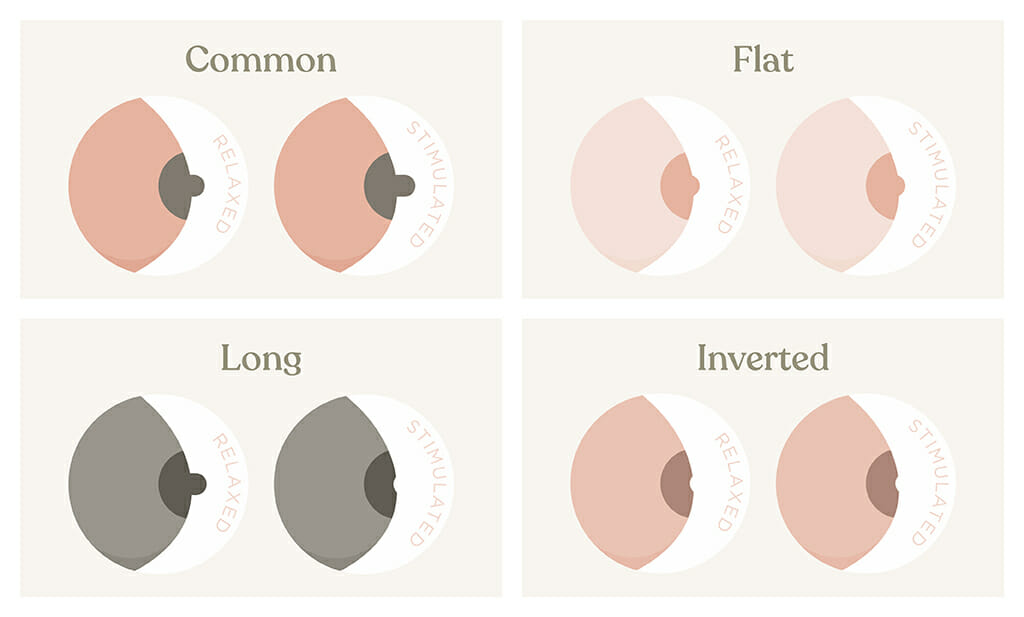
You have probably heard that there are different shapes of nipples: Flat, inverted, and long nipples. It is important that you really latch on correctly with these nipple shapes. Your baby doesn’t know any other shape and in most cases will have no problems with them. For example, before breastfeeding you can pump briefly to make the nipple stand out a bit more. Tools like nipple shapers can also help. Please keep the nipple clean and dry and do not use nipple shields. If you need to feed, only use a spoon or cup.
Unfavourable weight development in your child: Your child should not lose more than 7% in the first few days. In the case of exclusively breastfed children, the low point is usually reached on the third day. However, the birth weight should be reached again by the 10th day, or the 14th day at the latest. As a guideline, your child will then gain about 30 grams per day. What can you do to promote this? Skin contact, breastfeeding as needed, and at least every two hours – four hours off at night is okay. It is important to offer both breasts in different breastfeeding positions each time, not to use artificial teats, or give formula first in case of breast milk shortage, but contact your midwife, lactation consultant or paediatrician and ask for help.
Excessive onset of copious milk production: This causes sore and tense breasts and is caused by increased blood flow, onset of copious milk production and lymph congestion. Frequent and correct breastfeeding is preventive. What can you do? After breastfeeding, use cooling compresses for at least 20 minutes, e.g. frozen peas/corn, cool pack from the fridge, not the freezer compartment. Important: Always put a cloth between the pad and your breast. You can also perform a breast massage according to the breastfeeding counsellor’s instructions.
Newborn jaundice: A rise in jaundice levels up to a certain limit is normal in the first 5-7 days. If it is too high, it will be checked by the midwife or paediatrician and your baby may need to be treated with light therapy. Breastfeeding as needed and early first lactation have a preventive effect.
Insufficient milk production: Lack of milk is the reason for premature weaning for one third of women. However, over 95% of women are physically able to breastfeed their child sufficiently. Therefore, always consult a lactation consultant IBCLC or midwife and do not give up immediately.
Excessive supply of breast milk: This can lead to swallowing, changes in sucking behaviour, repeatedly letting go of the breast, crying and rejection. Further consequences can be milk congestion, breast infections and early weaning. Often the amount regulates itself after a few weeks. In any case, a specialist should be consulted. Sage tea and cooling the breast after breastfeeding can also have a milk-inhibiting effect.

Milk engorgement and breast inflammation: Here there is pain, hardening, redness, fever and discomfort. Please contact your midwife or breastfeeding counsellor. In case of milk engorgement, please seek medical treatment after 24 hours if the symptoms worsen!
All of the above reasons can lead you to give up breastfeeding prematurely, even though it not only offers your child the best nutrition, but also strengthens your bond and has a positive influence on its development. Therefore: Seek advice from a professional early on – breastfeeding should neither hurt nor be a struggle. An experienced lactation consultant can most likely help you save your breastfeeding relationship.


